Presented By
Dr. S. Das
Dr. Lily Proctor
Dr. Linda Hoang
Dr. Mark Carey
Dr. Neeraj Mehra
Dr. A. Shan
Affiliations
University of British Columbia
See full transcript here:
https://cansagevideos.com/hysteroscopic-resection-of-low-grade-early-stage-endometrial-cancer-in-a-patient-desiring-fertility-preservation
Hysteroscopic resection of an endometrial cancer for fertility preservation. Standard treatment for endometrial cancer consists of hysterectomy and BSO, which may not be acceptable for patients who wish to preserve fertility. Conservative treatment uses progestins. Our objective was to evaluate the feasibility and safety of hysteroscopic resection of a grade one endometrioid endometrial adenocarcinoma in the setting of desired fertility sparing management.
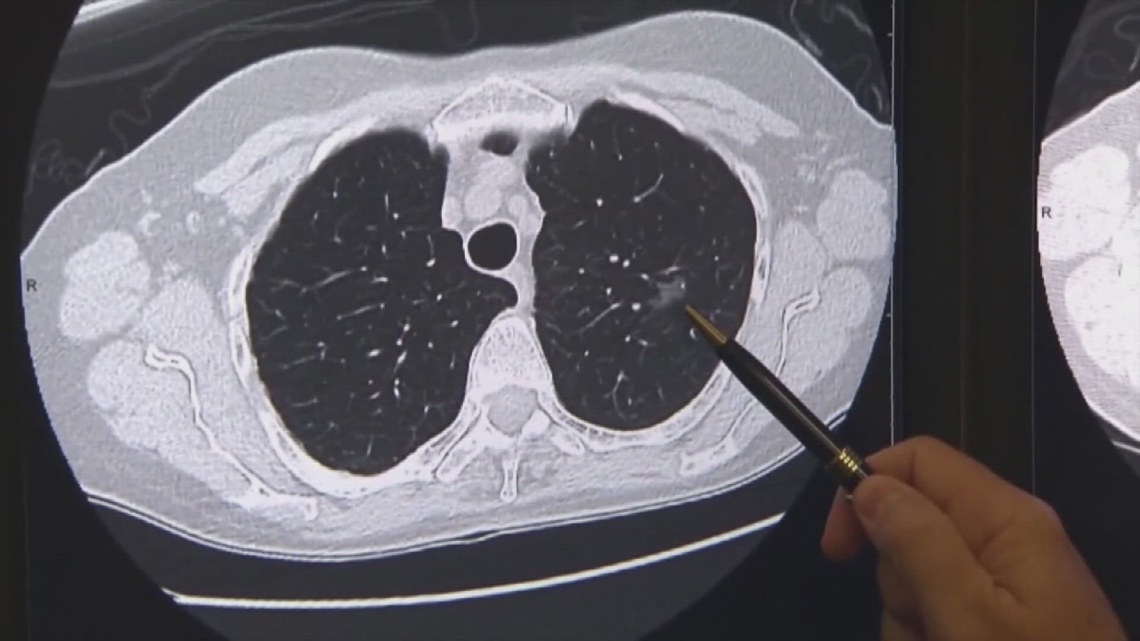
We had a 38-year-old Nullip who presented with endometrial adenocarcinoma. She strongly desired fertility and declined a hysterectomy BSO. An MRI was arranged showing a two cm fundal mass with a four mm invasion into the underlying junctional zone without serosal surface contact. Concomitant laparoscopy was an essential part of this operation as the resection was carried out deep into the myometrium with the risk of perforation.
The OR setup allowed both the primary surgeon and the assistant providing laparoscopic guidance the ability to see both the hysteroscopic and laparoscopic images. She was on progestin for four months to allow better visualization of the endometrial cancer. The uterine cavity was surveyed, and the mass was arising from the left fundus close to the cornea. The tumour was resected using a resectoscope in layers with the intention of a systematic analysis of each layer by the pathologist. The tumour was irregularly shaped and pale.
Pathological analysis of the first layer revealed entirely tumour. Further systematic resection was done. In the second layer, the gross appearance of the tumour was similar to layer one. On pathology, layer two showed both tumour and some myometrium. One of the challenges is that it is largely unknown what the appearance of endometrial cancer is on hysteroscopy. At the third layer, the myometrium, which is normally white in colour, still had areas of pink. We postulated this to be tumour.
Similar to layer 2, there were both areas of tumour as well as myometrium. The location of the disease made it challenging to obtain a good angle. The resectoscope was used to push and test the uterine wall to help determine depth. Laparoscopically, the camera light was kept at 40% intensity to allow transillumination. During resection the assistant also helped to hold the uterus away from the pelvic side wall. Laparoscopically, cautery effects could be seen on the surface of the uterus.
The deep margins were not possible as by this point, we were approaching the serosa, with a significant risk of perforation. The blood loss was 50 cc’s and the fluid balance was 400 cc’s. The visualised depth of invasion at hysteroscopy was deeper than what was seen on MRI. As the invasion at this point seemed to be greater than 50% of myometrium, the patient would be stage 1b. Also, cautery artifact as shown in this disrupted gland did not allow proper analysis of layer four.
Furthermore, there was a concern that there could be residual deep disease and for these reasons the patient was counselled on having a hysterectomy. The conventional pathologic examination of uterine specimens at our centre involves taking a rectangular cut of the uterine endometrium, as shown in the black box. In addition, we specifically asked the pathologist to examine the left cornua where the malignancy was known to be, to ensure areas of deeper invasion would not be missed.
On the hysterectomy specimen, no residual malignancy was seen, indicating success of the initial hysteroscopic resection. Our case demonstrated that hysteroscopic resection with high dose progesterone is feasible and may be an option for women who desire fertility sparing management of low-grade, low-stage endometrial cancers. Future prospective studies are required to determine the oncologic and reproductive outcomes.




![Angela Jay, former Page 3 star, dead at 71 after short cancer battle [Video]](https://crowd-funding.givetaxfree.org/wp-content/uploads/2024/05/mp_261095_0_SEI2028389261e8fe17149878964721714991745jpg.jpg)
![R&B Singer/Songwriter H.E.R. Celebrates Mom Being Cancer Free! - BlackDoctor.org [Video]](https://crowd-funding.givetaxfree.org/wp-content/uploads/2024/05/mp_261290_0_GettyImages1463263526jpg.jpg)